

Simplified Process
Our proven guided surgery system provides doctors with a streamlined approach that offers the best results.
No Required Fees
You will never be required to pay for planning or additional scanning fees with Guided Surgery Solutions.
Expert DMD Oversight
Unlike other surgical guide companies, we have expert doctor oversight for your cases.
Start Your First Case Today
Expert DMD Oversight to Assist You with Your First Case.
Feel free to give us a call at (855) 484-3335
Advanced Accuracy with a Simpler Guided Surgery System
Experience the Systematic Difference in Quality, Service & Support
Not Just a Surgical Guide:
A Proven, Systematic Solution
- Superior Design and Expert Service
- Innovative Solutions for Difficult Cases
- No Hidden/Mandatory Fees: Scan/Plan/Conversion
- No Investment in Software/Guided Instrumentation
- Expert DMD Oversight and Consultation
- All Implant Systems Addressed
Latest News
18Oct
How to Create an Accurate Alginate Impression
0 CommentsThe fit of the drill guide on the patient’s teeth is dependent on the quality of the stone model and,... Read More →
23Sep
Accuracy and the Perfect Pilot™
0 CommentsCreating a pilot osteotomy is a crucial step in guided surgery. If the trajectory of the pilot hole is off,... Read More →
22Sep
7 Things to Look for in a Surgical Guide
0 CommentsIt is important to note that not all guides are created equal. Intuitively, one might think that any guide is better... Read More →
08Sep
Immediate Extraction / Oblique Surface Surgical Sites
0 CommentsThere are particular challenges with immediate extraction and drilling into oblique surfaces that have the potential for significant error. Drilling... Read More →
13Aug
Differentiating Your Practice
0 CommentsHow does guided surgery differentiate your practice? Patients feel confident knowing that the surgeon has complete knowledge of all anatomy... Read More →
30Jul
How to Eliminate “Wag”
0 CommentsWhat is “wag”? – Wag is the radial movement of the drill tip due to the movement of the drill stop... Read More →
02Apr
How to Easily Find your Guided Surgery Protocol
0 CommentsEasy-to-use Protocol Selector Pick the right protocol before you start a case and you will never have to get a patient... Read More →
Contact Us
Our guide system is affordable and cost-effective – and we are as transparent on our pricing as our ThinLayer system. No hidden, mandatory conversion or planning service fees – complemented by no need to purchase an expensive guided instrument set and use of high quality free implant planning software.
Our streamlined data acquisition processes using CBCT and related FutureTooth™ information provides high accuracy and ease to facilitate detailed implant treatment plans and subsequent guide system design. Co-founded by a practicing periodontist, Guided Surgery Solutions leads with a focus on clinical quality and design from data acquisition and treatment plan through to guide QC. Our expert clinicians are proactive in review as well as guided surgery treatment planning and surgical technique.
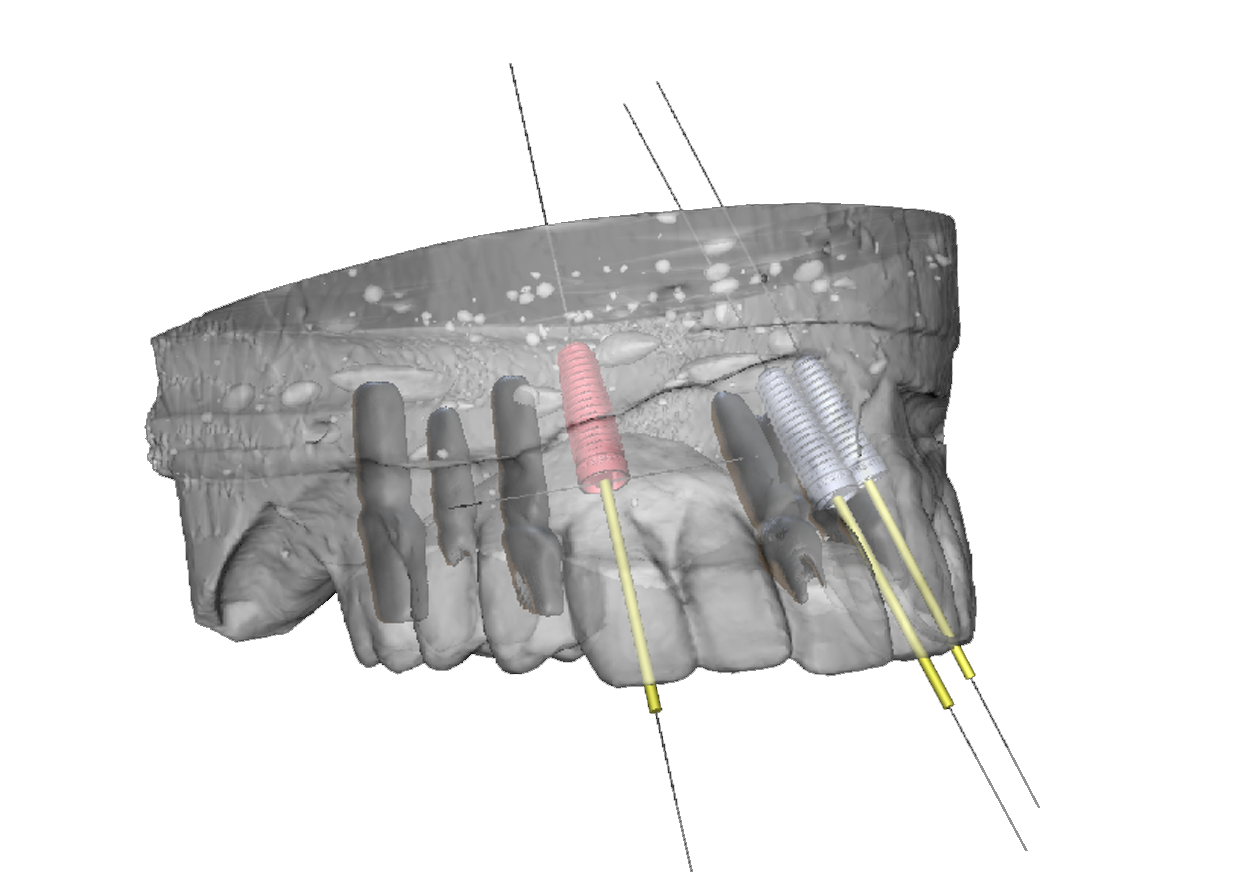
Designed to YOUR handpiece and drills, the ThinLayer® guided surgery system and related technique is efficient and delivers high quality, consistent guided surgery even in challenging cases.
“I learned as much planning my first case as I did during my residency. I don’t know why schools don’t teach this more!”
“I’m so glad I found your website… Every time I do a guided case, I tell myself I wish I could use it more often.”
Comments are closed.